
HIV Stigma and Discrimination: We Have the Power to Change the Conversation
Part two of a series to fill your kete with tools to be an informed ally when it comes to HIV stigma and discrimination.
Read part 1: HIV Stigma and Discrimination
Contents:
Stigma and discrimination: A recap
As we saw in Part 1 of this series:
- Stigma relates to how we think
- Discrimination relates to how we act
HIV-related stigma is often rooted in our belief systems from a young age. Becoming aware & tackling our unconscious bias and behaviours are the best ways we can use our power as allies to stand up to HIV stigma and discrimination at all levels of society.
People Living with HIV stigma index
People living with HIV face stigma and discrimination from all levels of society in their daily lives Think we’re exaggerating? Check out the latest Aotearoa New Zealand People Living with HIV Stigma Index reports to understand the current and very real experiences of people living with HIV.
All of Aotearoa New Zealand Māori people living with HIV“HIV-related stigma and discrimination can be seen in all levels of society.”
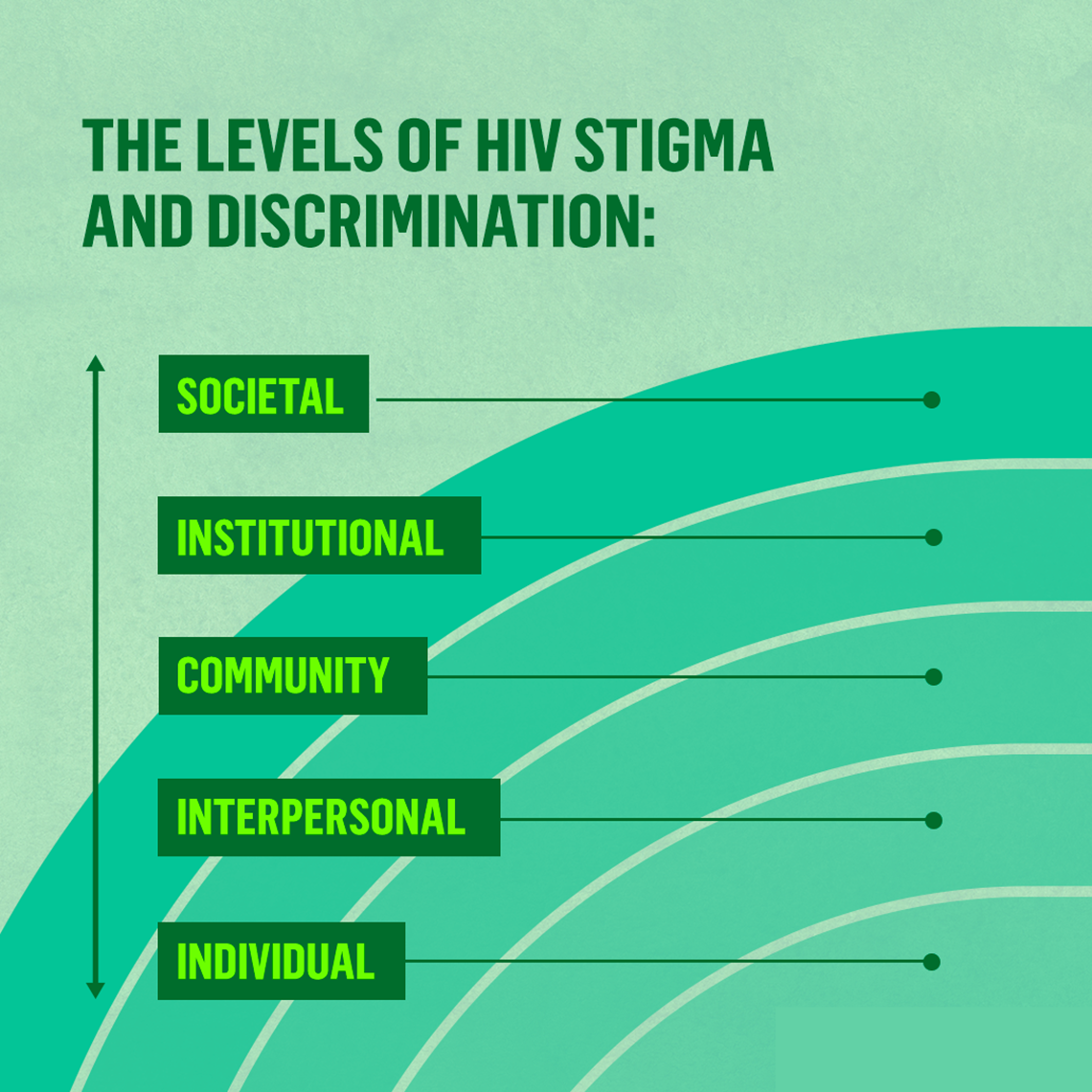
HIV-related stigma and discrimination in society
The diagram above illustrates how not only are we impacted by the attitudes and beliefs about HIV held at a societal level, but also how we play a role in influencing those same attitudes and beliefs. They work both ways.
At the individual level
We all hold personal beliefs about HIV. HIV-related stigma and discrimination at an individual level is often due to personal lack of education or awareness about HIV. This can impact our own behaviours, but can also influence those closest to us.
At the interpersonal level
We can also learn and stand up to HIV-related stigma from the people we are closest to – our friends and whānau. Think about the last time that HIV came up in conversation with a loved one. What was their attitude about HIV? How did you respond?
We don’t always consciously recognise this at the time (i.e. a child may grow up with a parent who holds a certain belief and doesn’t consciously question it). Even if we do recognise it, it’s often hard to challenge (i.e. you may decide not to speak up about your partner’s views for fear of damaging your relationship).
The dominant viewpoint is typically held by those who have the most power in the relationship. This is how HIV stigma can be perpetuated.
“Think about the last time that HIV came up in conversation with a loved one. What was their attitude about HIV? How did you respond?”

At the community level
HIV-related stigma and discrimination can also be seen in the communities we’re connected to.
Communities are made up of many interpersonal relationships between friends and whānau members, therefore the dominant viewpoint of interpersonal relationships also comes into play. If there are enough influential viewpoints on a topic such as HIV acceptance, this viewpoint can be accepted and adopted by the wider community.
While a community is likely to have a variety of opinions on certain matters, it’s usually large enough to protect the dominant viewpoint and alienate those who don’t share that view.
What do we mean by ‘community’?
Communities are made up of people who have something in common; perhaps they all have children at the same school, are part of the same iwi, go to the same church, or are of the same ethnicity.

At the institutional level
Our society is shaped by key institutions. The weight of dominant beliefs and ideologies within communities throughout our society plays a huge role in how our institutions advertently or inadvertently perpetuate HIV-related stigma and discrimination.
These can play out differently in different institutions. For example, governments may pass laws criminalising HIV transmissions, healthcare professionals may choose not to treat patients who are living with HIV, or media organisations may broadcast TV shows that perpetuate negative ideas about HIV.
Positive Speakers Bureau
The Positive Speakers’ Bureau is New Zealand’s preferred supplier of HIV education services. They empower people living with HIV to share their stories, raise awareness, and improve the knowledge and understanding of HIV throughout the country.
Learn more about the Positive Speakers BureauAt the societal level
The beliefs that are perpetuated at an institutional level play a massive part in how we as individuals operate within society.
When we see consistent messages about HIV echoed throughout governmental decisions, the media we consume, and the behaviour of our healthcare professionals, it can take a long time to even become aware of them, let along do anything about them.
For example, if the films and television shows you watched as a child consistently suggested that most gay people had HIV and that they often died from it, you may have grown up never questioning whether or not this was accurate.

Internalised HIV stigma
As we learnt in Part 1, people living with HIV can and often do experience internalised HIV stigma. The effects of this is also seen and felt through every level of society:
- Individual: Internalised HIV stigma can lower someone’s feelings of self-worth, increase the risk of mental health issues such as depression and anxiety, and make it more difficult for them to seek help and treatment.
- Interpersonal: Someone’s internalised feelings about their own HIV status can impact on their relationships with those closest to them. People living with HIV may fear transmitting HIV to a partner (those who know they have an undetectable viral load can also feel this fear as the internalised stigma can override their logic functions), or they might worry how a disclosure of their HIV status may impact a relationship.
- Community: Internalised HIV stigma can make someone feel isolated from their community. However, a community can also be found amongst peers of other people living with HIV and services that support them. Studies have shown that a connection to other people living with HIV helps to reduce internalised HIV stigma.
- Institutional: While it’s everyones’ responsibility to advocate for an equitable society, unfortunately it often falls to marginalised groups to advocate for changes that specifically affect them. Internalised HIV stigma corrodes peoples’ ability to do this effectively because they hold the same stigma that they are experiencing.
- Societal: Internalised HIV stigma can inhibit stigma reduction in key institutions, and it’s much harder for society to change if institutions don’t.
Leading the way
Despite internalised HIV stigma, many people living with HIV have become beacons of home for their community. Here’s some groups and individuals that you need to follow.
HIV activists you need to follow“Studies have shown that a connection to other people living with HIV helps to reduce internalised HIV stigma.”

With great power comes great responsibility
So, what can you do about HIV stigma? As you can see, beliefs and behaviours regarding HIV that we see play out in society have an immense impact in how we individually think and feel about HIV.
However, on the flipside, those societal beliefs and behaviours are made up of the beliefs and behaviours of our institutions, which are ultimately influenced by individual people.
Us.
You.
That’s right; your own individual beliefs and behaviours have the power to change the way that society itself views HIV.
Some questions to ask yourself:
- What knowledge do I have about HIV? For example, do I understand the difference between HIV and AIDS?
- Am I aware that I could have condomless sex with someone living with HIV and not contract HIV due undetectable viral loads (keep scrolling for more info)?
- Do I know anyone who is living with HIV?
- Have I heard their stories?
- Am I aware that there may be other people in my life who are also living with HIV without me realising it?
- How does that make me feel?
Answering these questions honestly will give you a good indication of how much HIV-related stigma you hold. The best thing you can do as an individual is get educated on HIV to ensure that your stigma doesn’t contribute to societal stigma.
The good news is that this works both ways. Deliberately breaking down stigma at an individual level can influence society in the same way as stigma itself. We all have a role to play in how our society functions. But with great power comes great responsibility.
What are you going to do with it?
Undetectable = Untransmittable (U=U)
HIV medications work by reducing the amount of virus in the blood to a very low level where it can't be detected by a standard viral load test. Having an undetectable viral load also means HIV can't be passed onto sexual partners. We call this ‘Undetectable = Untransmittable’, or ‘U=U’.
“Ki te kotahi te kākaho, ka whati; ki te kāpuia, e kore e whati”. If a reed stands alone, it can be broken; if it’s in a group, it cannot”.

Next up in the series
Discrimination can have many faces, some of which are very hard to recognize. Next up, we’ll explore some common concrete examples of what HIV-related discrimination can look like. Once we know what we’re looking for, it’s a lot easier to do something about it.
Read part three: How to recognise HIV-related stigma and discrimination
To sum up
- HIV-related stigma is how we think, and HIV-related discrimination is how we act
- HIV-related stigma and discrimination can play out in all levels of society
- Internalised HIV stigma works in exactly the same way
- We can be incredibly influenced by the beliefs that are perpetuated at a societal level
- But we also have the power to change those beliefs at an individual level
- Once we understand this power, we have a choice; will we sit back, or will we choose to make a difference?